Last Updated on February 26, 2025 by MASSAGE Magazine
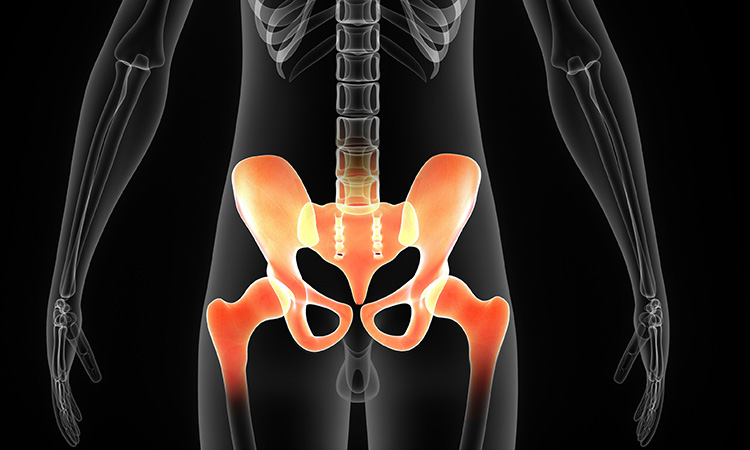
Understanding anatomy of the hip joint is integral to understanding musculoskeletal dysfunction because of its influences not only at the pelvic girdle but above and below the pelvis as well.
The ball-and-socket joint of the hip, or the acetabulofemoral, joint allows for a wide range of movement, which makes possible important daily activities such as walking, squatting, running and jumping.
Actions at the hip joint include extension, flexion, adduction, abduction, internal rotation, external rotation, horizontal adduction and horizontal abduction. Combinations of these movements propel us through the world every day.
Weight bearing is another important role the hip joint provides for the system. Unlike other ball-and-socket joints like the glenohumeral joint or shoulder joint, the hip joint is often, throughout the day, placed in a weight-bearing capacity.
Therefore, the hip joint not only provides mobility for the body, but stability as well. Strong capsular ligaments and complex muscle activation allow the hip to carry our weight as we move through space.

Forces are applied to the acetabulofemoral joint from our body weight (forces from above, downward) as well as the ground reaction force (forces from below, upward). In the complex system that is human bipedalism, the hip plays a starring role.
Full Mobility
Given the architecture and functional importance of the hip joint, full mobility is essential.
If the mobility in the hip is limited, that limitation in range of motion has to be compensated for elsewhere. In one recent study published in the International Journal of Sports Physical Therapy, “Passive hip range of motion is reduced in active subjects with chronic low back pain compared to controls,” loss of hip extension was shown to correlate with the presence of chronic low-back pain.
What the hips cannot do, the low back will try to make up for, leading to musculoskeletal pain and dysfunction. While the low back may be hypertonic and tender to touch, the larger question is why. Range-of-motion testing of the hip may reveal that the low back is doing too much. In that case, treatment focused only on the low back is not likely to be successful, no matter what the intervention.
Compensation for restricted hip mobility can also spread down the kinetic chain, as exemplified by a study published in Knee Surgery, Sports Traumatology, Arthroscopy, “Restriction in hip internal rotation is associated with an increased risk of ACL injury,” which showed loss of internal rotation of the hip was correlated with knee injuries, specifically to the anterior cruciate ligament (ACL).
Decreased strength or lowered hip mobility around the hip is bound to disturb normal gait patterns, likely leading to altered biomechanics and thus possible dysfunction throughout the kinetic chain—and complaints from head to toe.
Seeking Balance
Identifying decreases in range of motion can be an important tool for massage therapists to help determine possible sources of pain. To test range of motion, the client should wear comfortable, loose-fitting clothes.
The therapist needs to be aware of both quantitative and qualitative criteria during passive range of motion testing, assessing not only how far (quantitative), but also paying attention to how the body responds to the movement (qualitative), especially at the end of range, called end feel.
If the end feel is flexible and elastic, the restriction is probably soft-tissue in nature. If the end feel feels excessively hard, as if you are hitting a wall you cannot push past, that is a possible sign of intrajoint pathology, such as arthritic changes.
Deep knowledge of functional anatomy is a prerequisite for fully utilizing range-of-motion testing. When testing any plane of movement, you are length-testing muscles that do the opposite action. For instance, testing internal rotation of the hip is length-testing the muscles that create external rotation. Obviously, it is important to know what those muscles are and then have the skill set to address each of them precisely and thoroughly.
Furthermore, it is important to note that excessive range in any plane is not necessarily beneficial, especially if it is in one plane of movement only. These asymmetries are often problematic, often more so than symmetrical restrictions. Therapists are likely to discover that after increasing flexibility in a restricted plane, the opposite plane—which was previously hyperflexible—will now decrease in range. The body tends to seek balance.
Range-of-Motion Tests
Internal and external rotation can be tested in both supine and prone positions. To test internal rotation from the supine position, use the 90/90 position, which means the client’s knee is bent at 90 degrees and the hip is flexed to 90 degrees as well.
Taking the foot and lower leg laterally allows the acetabulofemoral joint to rotate internally. The hip should be able to rotate internally approximately 40 degrees. This can be measured with a goniometer or estimated visually.

To test internal rotation in the prone position, the knee is again flexed to 90 degrees so the foot is above the knee. The foot is then moved laterally again so the femoral head can rotate internally within the acetabulum. The therapist should place one hand on the pelvis or sacrum.
The end of range is revealed when the pelvis or sacrum begins to rise, signifying the end of independent motion of the femur relative to the pelvis.
External rotation can be done in both supine and prone positions as well and involves the opposite motion with the femur. In the supine position, employ the same 90/90 position of the hip and the knee. To test external rotation, take the lower leg and foot medially, rotating the femur externally. The ideal range of motion for external rotation is approximately 60 degrees.
To test external rotation in the prone position, the knee is again flexed to 90 degrees so the foot is above the knee. The lower leg and foot is then moved medially, rotating the femoral head externally within the acetabulum. Monitoring the pelvis with one hand, the end of range is revealed when the pelvis or sacrum begins to rise.

Testing flexion of the hip is accomplished with the client supine. With the knee above the hip, bring the knee as far toward the chest as is comfortable for the client. Flexion should be approximately 40 degrees from the starting position.
Hip flexion is not usually limited; if it is the therapist should be aware of a hard end feel, because limited flexion and hard feel may be indicative of hip joint pathologies. When flexion is limited past the 90-degree starting position, the other leg will often be lifted off the table (the knee will bend), being pulled by rotation of the pelvis as a whole.

In testing hip adduction, you are testing the length of the hip abductors. With the person in side-lying position, have the shoulders, hips and knee all in a straight line. Supporting the knee with your hand, lower the leg with one hand while monitoring the movement of the pelvis with the other hand. When you sense with your superior hand the pelvic crest being pulled inferiorly, this is the end of range of motion. Optimal range is that the tested knee will travel halfway to the table.

To test abduction, you are length testing the adductors of the hip. With the client supine, abduct the leg while monitoring the opposite anterior superior iliac spine (ASIS). The moment the ASIS dips inferiorly reveals the end of range. Two helpful hints are: Don’t move too slowly, as speed makes the end of range easier to recognize; and keep the leg in a neutral position.

Extension is measured prone with the knee flexed and the foot above the knee. The therapist lifts the femur from the knee toward the ceiling while monitoring any movement in the pelvis and sacrum. The acetabulofemoral joint should extend 30 degrees before the sacrum and pelvis begin to move. If the person experiences back pain while doing this, consider the psoas muscle as a possible source.
Hip extension restrictions are commonly overlooked and often unnoticed by the client, yet it may be one of the first signs of hip restriction. This plane is often limited for people who spend a lot of time sitting.
Finding that the hip is restricted in extension is important, but it would be helpful to know exactly which muscles are causing that restriction. To discover which muscles may be causing hip extension restrictions, you may employ a modification of the Thomas Test.
With the client in supine position, have the knee on the untested side bent and that foot resting on the table. Raise the straight leg on the side you are testing to about 50 degrees. With your superior hand, monitor the inferior surface of the ASIS.
As you lower the leg, monitor any movement of the ASIS. Full range is accomplished when the leg makes it all the way to the table with no movement in the ASIS. Muscles to suspect if the ASIS is pulled inferiorly are the iliacus, rectus femoris and tensor fascia lata.

These specific range-of-motion tests can provide clues as to possible reasons for your clients’ presenting symptoms. While range of motion is important, full range is not the answer to every problem. The authors have seen many clients with full range and significant discomfort. In the complex world of musculoskeletal pain, range is but one criterion—but one worth considering as a possible source of your client’s pain.
About the Authors:

Douglas Nelson, BCTMB, LMT, is celebrating his 43rd year in clinical practice and is the current president of the Massage Therapy Foundation (MTF). His articles for this publication include “Geriatric Massage: Why Touch is so Important as We Age.”
James Ivaska started his career as a massage therapist after receiving his master’s degree in kinesiology. He is the owner of Muscular Health Center in Alexandria, Virginia and teaches for Precision Neuromuscular Therapy Seminars.