Last Updated on June 12, 2024 by MASSAGE Magazine

One of the more commonly misunderstood use of terms I have observed in the massage profession is sciatica. Depending on how we are trained, what our clients tell us they have been diagnosed with, and the location of the pain the client is complaining of, many people are confused about sciatica versus piriformis syndrome.
Even as an educator, I have interchanged these terms simply due to the relationship of the anatomical location of the hip, piriformis and sciatic nerve.
However, it is important to understand the difference between these two pain issues. This distinction lies in what is putting pressure on the sciatic nerve and the location in which the pain is originating.
Sciatica Versus Piriformis Syndrome
Sciatica is a symptom of a herniated or bulging disc in the spine pressing on the sciatic nerve. Also called lumbar radiculopathy, it is pain that originates along your sciatic nerve. It’s a symptom of an underlying condition, not a diagnosis.
Sciatica most commonly occurs in people between the ages of 30 and 50 years, and while it is mainly credited to a bulging disc it can also be attributed to obesity, poor posture, awkward sitting positions or nerve disorders.
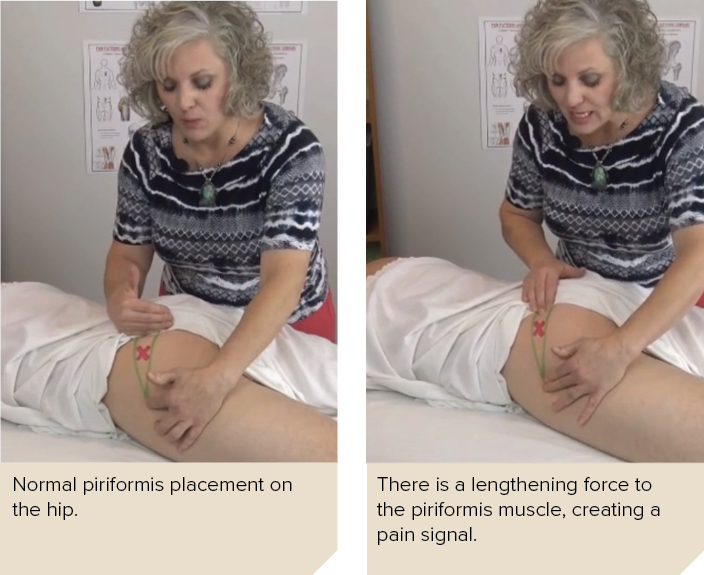
Piriformis syndrome is a condition in which the piriformis muscle, located in the buttock region, spasms and causes buttock pain. The piriformis muscle also can irritate the nearby sciatic nerve and cause pain, numbness and tingling along the back of the leg and into the foot, similar to sciatic pain.
Causes of piriformis syndrome typically begin with an injury or injury response and include a tightening of the muscle, spams, or swelling of the area that then affects the nerve.
What we typically observe comes across our massage table is more of a chronic version of piriformis syndrome with sciatic irritation that is referred to as sciatica.
Dealing with Chronic Piriformis Syndrome Pain
Regardless of what this pain is called, our clients point to their backside and ask us to use our elbows, fists or knuckles to dig at their hip and buttocks for some relief of the muscle and nerve pain they are experiencing.
I think this is where massage therapists really shine in the ability to spend the needed time and attention on an area of pain using trained, competent touch.
Many times, a simple combination of direct and correct pressure on the afflicted piriformis, attachment site work, stretching, or even using as strain-counterstain style of bodywork, (not to mention all the other wonderful techniques available at our fingertips) many clients experience tremendous relief.
But what do we do when clients’ pain increases, inflames and does not respond to a direct therapeutic approach for piriformis pain and many other pain issues?
Treating Inflammation First; Pain Second
Having been trained as a neuromuscular and trigger point massage therapist, I have had a passion for working with pain management for quite some time. As I progressed into my career, I saw that my clientele naturally sorted themselves into two types of clients that I began calling Client A and Client B.
Client A were those clients that responded beautifully to the therapeutic inflammatory techniques I applied. Client B were those whose bodies rejected most approaches, would inflame more with very little application, and increase in pain regardless of how I altered my techniques.
I became interested in why client B was not responding and the answers to non-responsive pain became my lifelong study. The best approach I have learned is to figure out what would take the most pressure off that specific afflicted muscle or tissue that would then allow it to rest and heal.
Client B is experiencing higher levels of inflammation that dictate what I am allowed to do or even what I am allowed to touch. That makes it difficult when a client desperately want you to deeply address a painful area but in doing so, it perpetuates their pain further. Even though addressing the pain is the focus for both the client and myself, decreasing inflammation is the requirement to then have access to pain relief.
And therein lies the delimma: How do we apply pain-relieving massage to an area that we canot actually touch but need to, in order to create a pain-reducing affect and make sure the client feels true pain relief?
My experience has taught me that sometimes the further away I look from the issue proves to be a better answer, and that equal and opposite reactions mean that many solutions could be found within the identical twin to the tissue in pain (for example, bicep to bicep).

The Indirect Approach for Piriformis Syndrome
For piriformis syndrome, the simple pain pattern solution is to work with the opposite piriformis but not specifically the muscle itself. What I have observed is that there is a chain reaction or a line of force that travels from one hip, through the piriformis muscle, across the sacrum, through the opposite piriformis muscle, and then to the opposite hip.
There are two main anchoring points in this line: the boney surfaces of the femurs, the surrounding ligaments, and broad pieces of fascia (IT Band).
The side that started this line of force and adhering was typically the side not in pain.
The process looks more like one posterior and lateral hip area gets stuck, then the opposite hip in the same place (equal and opposite reactions) and then somewhere in the middle of all of that, specific muscles become over-stretched and that is the pain the client complains of.
I see this looking like a game of tug-o-war, the piriformis in pain is the point of greatest strain in the middle of the two pulling sides—only in this instance, the middle is tearing and is in pain.

• To reverse this chain reaction, locate the insertion of the unaffected piriformis on the head of the trochanter and work directly on the trochanter at the attachment site and the surrounding tissue.
The other tissues included with this application are:
• The posterior aspect of the IT Band at the level of the hip and Ischial Tuberosity along with the gluteus maximus attachments
• All around the interfacing boney areas of the femur and head of the femur located under the IT Band looking for areas of adhesion
• Directly on top of the Sacral Tuberous Ligament as it travels inferiorly from the sacrum to the Ischial tuberosity and then again on top the Ischial tuberosity
• Any shortened or adhered tissue between the ischial tuberosity, IT band, Sacrotuberous ligament, at the level of deep hip rotators.

Then, repeat this work to opposite side, looking for adhesion along the bone and ligaments. Avoid deeply working deeply on the piriformis muscle this session. Finish this approach with a soothing application of touch to the muscles of the hip in pain, realizing that the muscle needs time to heal before it can respond to direct force.
Lastly, one of the realizations I have had with Client B and their body is that these types of patterns occur from injuries. Even though the description of the pain from clients sounds the same, what is causing the pain is not. That is biggest difference between Client A and Client B.
Client A has more of a compensation pattern occurring from things such as overuse and the muscles need to be worked to respond and regain health. Client B has an adherence issue with several involved tissue including ligaments and fascia that are typically bound into a specific location. A past Injury is almost always involved to create the chain reaction as outlined above for the piriformis.
Interestingly enough, the work for client B does not work with Client A. Just like the work I was doing for client A would not work for client B even though the pain appears the same.
The reason it is there is different and so is the level of inflammation based on those reasons. This is one of the explanations for why inflammation seems unbridled with these bodies. Inflammation must be resolved first, with the muscles being given a chance to heal before the pain can be truly resolved.

About the Author
Amy Bradley Radford, LMT, BCTMB, has been a massage therapist and educator for more than 25 years. She is the owner of Massage Business Methods and the developer of PPS (Pain Patterns and Solutions) Seminars CE courses and an NCBTMB Approved CE Provider.