Last Updated on August 29, 2024 by MASSAGE Magazine
In the early 1990s, I had the opportunity to study with legendary neurologist and physiotherapist Vladimir Janda, MD.
He and his research team at Charles University in Prague, Czechoslovakia, were among the first to perform EMG studies showing that some muscles weaken and others tighten when exposed to prolonged stress. In the course of their research, one unexpected length-strength muscle imbalance pattern appeared in people with forward head carriage (Fig. 1).
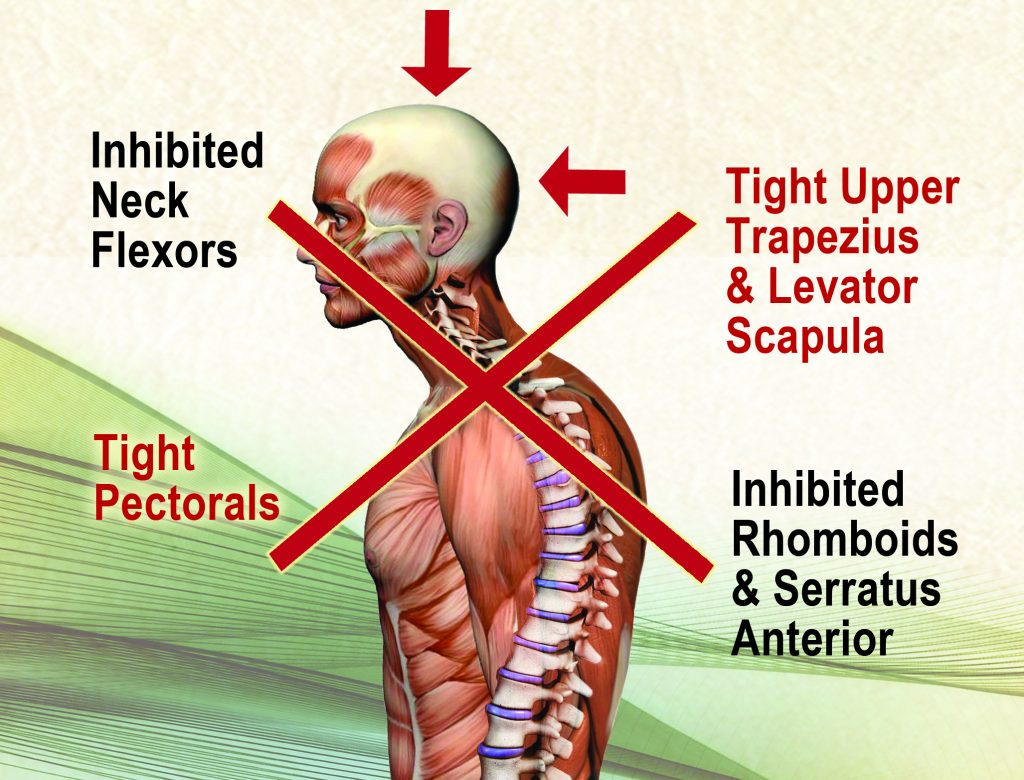
In the illustration, notice how the tight and weak muscles form a crossing pattern; Janda and his team called this Upper Cross Syndrome. In an effort to expound on Janda’s findings, my graphic designer and I created an image called “The 42 Pound Head” (Fig. 2). This shows how the feeling of head weight increases by 10 pounds for every inch the head moves forward from the shoulders.

Janda’s Upper Cross Syndrome muscle imbalance theory has become widely popularized as an easy-to-visualize assessment tool. However, it has met with harsh criticism from researchers who did not find the pattern to be a reliable marker of pain.
In an attempt to upgrade Janda’s research using current brain-based understandings, in this article I’ll review the evolution of upright head posture and discuss the neurologic role of muscular imbalance. I’ll also demonstrate myoskeletal graded exposure techniques I’ve found helpful in relieving postural stress, improving cognition and increasing body awareness.
A Wider Horizon
One of the evolutionary advantages of erect head-on-neck posture is that it establishes ease of head rotation around a vertical axis, which serves to widen our horizon.
In early man, the need to stabilize this sensory platform to track prey was essential for survival. Famed research anthropologist José Luis Alatorre Warren at the University of Zurich found that evolutionary changes in the size and positioning of the cranium largely resulted from adaptations necessary for bipedal upright walking.
To ensure optimal head-on-neck balance, the foramen magnum — the opening at the occiput for the spinal cord — was forced to migrate forward during human evolution. There are many possible explanations for why Mother Nature considers a balanced head so desirable for upright humans, but the most obvious one is improved visual tracking.
Head Orientation and Cranial Teleceptors
The human head houses sensory organs called cranial teleceptors that connect us to the outside world. When floating comfortably atop the spine, these intricate receptors reflexively orient head placement using light, sound and gravitational sensory information. In fact, our eyes must constantly move, via saccades (rapid eye movements), to allow light to traverse across the retina. This allows the central nervous system to construct visual images by comparing adjoining structures in our environment. Therefore, our brains are often unable to make sense of visual input without proper head-on-neck movement.
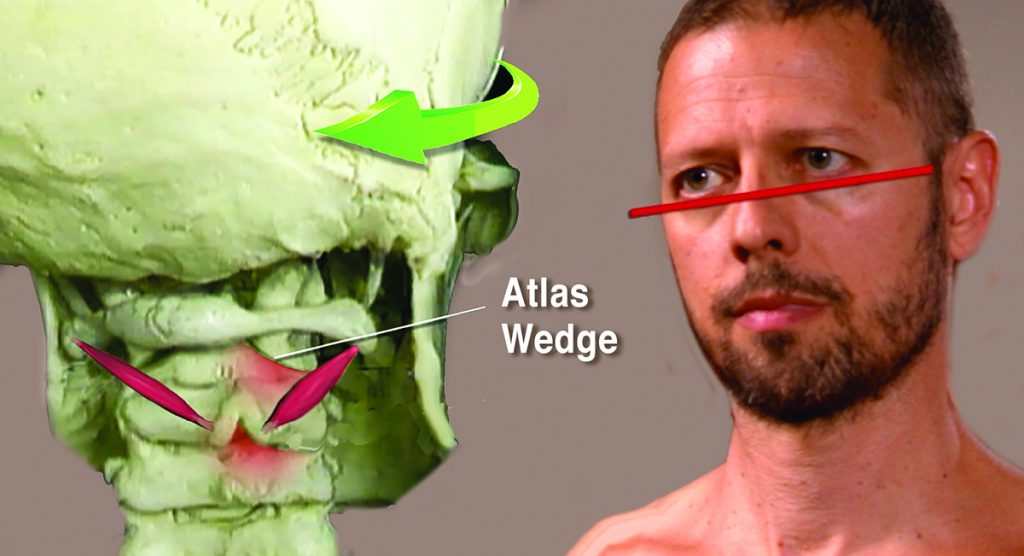
Unfortunately, teleceptor function is often compromised due to postural ergonomic stress, micro- and macro-traumatic events, and accompanying inflammation. In time, failure of the smooth self-regulating function of these receptors results in a catch-22 cycle, as faulty alignment initiates head-righting reflexes that trigger muscle spasm and mechanically alter spinal joint motion (Fig. 3).
As hyperexcited joint and ligament mechanoreceptors initiate protective splinting, some muscles overwork and others become neurologically inhibited, as seen in Janda’s Upper Cross Syndrome. This results in reduced mobility, excessive energy consumption, exhaustion and, if the brain perceives threat, pain.
However, such cranial teleceptor malfunction and head-righting reflexes may not be the only neurological explanation for the commonly seen muscular imbalance pattern Janda encountered in his Upper Cross Syndrome research.
The SAID Principle
The SAID principle — an acronym for Specific Adaptation to Imposed Demands — is a classic sports medicine term describing how physical adaptations develop when the body is placed under stress, thereby allowing us to better handle future stressors. Simply put, the body gets better at doing whatever it does regularly.
If that means sitting for hours in a desk-occupied posture or performing exercises using poor form, the brain will accommodate by adopting poor form and less-than-perfect posture (Fig. 4). I call this brain-body adaptation process postural plasticity and believe it to be a valuable assessment tool for identifying possible roots of suboptimal posture and inefficient movement.

Weak postural patterns such as Janda’s Upper Cross Syndrome may begin as tissue issues due to tension, trauma or overuse injuries, but eventually they manifest as signs of functional weakness in the brain’s hardware.
Pontomedullary Reticular Formation (PMRF)
The PMRF is a dynamic sorting and switching station located in the brainstem at the pontomedullary junction, where pons meets the medulla (Fig. 5). Considered the epicenter for postural control, the PMRF houses eight cranial nerves that perform vital sensory and motor functions, including vestibulo-ocular (eye and ear) coordination.

The PMRF is assigned the tasks of regulating head-righting reflexes, maintaining balanced gait and, when functioning optimally, inhibiting cervicothoracic flexion and resisting gravitationally-induced slumping.
Clients with bilateral PMRF disorders commonly present with Upper Cross Syndrome postural symptoms, such as forward-jutted chins, internally rotated arms, protracted shoulders and thoracic spine hyperkyphosis. In this population, the PMRF is unable to neurologically resist slumping, which leads to connective tissue and joint adaptations as seen in Janda’s model.
Assessment and Correction of Upper Cross Syndrome
It’s best to assess for PMRF weakness with the client unaware they’re being examined. I begin by observing my client’s posture and gait as they enter the office, looking for front-to-back and side-to-side rotational strain patterns that may indicate PMRF weakness.
Then, during the intake evaluation, I’m watching for things such as motor dominance patterns, eye unleveling and cross-lateral gait disturbances, which may offer clues to unilateral or bilateral PMRF weakness. I find weeding out these common compensatory patterns early on in therapy provides a good starting point for more specific assessment and treatment interventions to follow.
As shown in Fig. 6, I assess for unilateral PMRF weakness using a modified wall angel. The client is asked to side-bend around my finger fulcrum placed on his sternum while keeping his chin tucked and thorax and hands in contact with the wall. Notice that as he left side-bends, his shoulder and hand leave the wall and his chin juts forward. To help stimulate his postural reflexes and improve his unilateral PMRF weakness, I perform a graded exposure myoskeletal technique.

I begin by left-rotating and extending his head, abducting his arm and placing a soft palm on his chest wall. He is asked to slowly begin externally and internally rotating his arm while I apply hand pressure to various spots on his anterior shoulder and chest to bring awareness to areas of restriction (Fig. 7). Then, I retest for improved quality of motion. If the client had presented with bilateral PMRF weakness, I could have performed a cross-armed shoulder depression technique by asking him to inhale, protract his shoulders against my resistance to a count of five, exhale and relax (Fig. 8).


Repeating these novel movement enhancers several times using various amounts of hand pressure brings improved sensorimotor awareness, which helps convince the brain it’s safe to move through the soft tissue restrictions. Movement enhancers help the client resist slumping by strengthening the PMRF and stimulating postural reflexes. In addition, they encourage total body extension through activation of the vestibular system.
Vestibular System’s Extensor Response
The vestibular system’s inner ear houses organs that contribute to postural stability by interpreting changes in movement, direction and velocity. This complex balance center helps lift us against opposing gravitational forces by exciting ipsilateral motoneurons of the limbs and trunk while inhibiting the flexor motoneurons that cause us to slump (extensor response).
With a healthy PMRF resisting flexion and a highly functioning vestibular system promoting extension, our posturally challenged clients can stand taller and move better, which leads to improved cognition and teleceptor function.
Remember, the brain regulates tone in all the body’s connective tissues and can activate or inhibit muscle tone and balance depending on what it determines to be the safest course of action at that particular time. Much like an overprotective mother, it’s always making decisions on how much activation to allow while deliberately erring on the side of caution.
We are wired for survival, and our (Mom) brain is designed to support and protect us. When functioning properly, the brain knows when too much or too little of a good thing is just right.
Summary
Poor posture is not a cause as much as a symptom. Essentially, it is dysfunction of various bodily systems that are either over- or under-functioning. In most bodywork circles, we consider faulty posture a tissue issue, and in many cases, problems do arise from strained or overused connective tissues and joints.
When performing a postural assessment as part of a client’s intake exam, continue to address tissue issues such as Janda’s Upper Cross Syndrome pattern; but more importantly, try to determine what the nervous system is doing with this information. These patterns may have started as functional or pathological muscle imbalances, but left untreated, the SAID principle will trigger the brain’s hardware to begin memorizing and mapping these aberrant patterns as normal.
Always remember: The brain craves complexity. Repetitive, monotonous, uniplanar movements, such as those performed on health-club machines, are not only unhelpful in stimulating optimal posture and dynamic movement, but may also promote weak posture and unrefined movement patterns.
Using postural plasticity to create positive change through myoskeletal brain-based bodywork requires the addition of dynamic movement and active participation from the client at all times. I recommend novel home exercise therapy programs such as Paul Kelly’s PhysioKinetix Training to help enhance the hands-on work.
As sensorimotor integration is upregulated through good bodywork and corrective proprioceptive extension exercises, the client will notice a marked reduction of aches and pains while gaining improved body awareness, enhanced mobility and overall endurance. The goal of brain-based bodywork is to restore flexor-extensor synergy, postural stabilization and dynamic movement during daily living.
About the Author

Erik Dalton, PhD, developed Myoskeletal Alignment Techniques (MAT®), a hands-on bodywork system designed to restore function, relieve pain, rebalance the nervous system and re-educate the body. He has more than 30 years’ experience in educating massage therapists. Dalton’s courses are approved by the National Certification Board for Therapeutic Massage & Bodywork for continuing education. He is also a MASSAGE Magazine All-Star.